
My daughter, Rose, was born with Trisomy 18 — a rare genetic condition — along with congenital heart disease. Doctors labeled her diagnosis “incompatible with life,” and from the start, it became painfully clear how difficult it would be to secure full medical care for her both at birth and afterward. Many life-saving interventions are considered “futile” for children like her, so families are often told no. This is the story of how we fought for Rose’s life-saving care — told through a mother’s eyes — a journey of broken hearts searching desperately for healing.
“Mrs. Willard, can you have a seat right here?” Those simple words were the first crack in my safe, familiar world of pregnancy. I was naïve about genetic disorders and the way they alter everything — even access to care. Sitting alone in the waiting area after my sonogram, I texted my husband and my mom happily: “All done! Saw the heart, the sac, the tiny baby — everything looks normal.” I didn’t know it would be the last time anyone in medicine ever described Rose as “normal.”
Moments later, I was called back again. A staff member asked if I had completed genetic screening. I explained that I had — and heard nothing — so I assumed everything was fine. She simply asked me to follow her. My heart dropped. I felt like I had stepped into a roller coaster loading dock — strapped in, unable to escape, bracing for a drop I couldn’t see.
When the provider finally said, “There are concerning signs,” I sat completely still. I thought maybe it was about my age, or routine testing. For a brief moment, I felt peace — like somehow my child was still okay. But then came the words about a high-risk chromosomal disorder — not Trisomy 21 — “worse,” they said.

I was handed a packet. I was told this wasn’t a viable pregnancy, that I needed to meet the doctor immediately, and that “this diagnosis is not compatible with life.” There was time to make “a decision,” but not too much.
I walked out flushed and shaking, down the same hallway that had once felt joyful. Suddenly, I didn’t belong among the excited, glowing mothers. I sensed I would never be the same — and I wasn’t. The months that followed were filled with specialists, genetic counseling, and endless explanations to friends and family. I became a translator — carrying unfamiliar, heavy words from room to room.

Then came the question that pierced deeper than any doctor’s statement: “Why is she keeping it?” Coming not from a stranger, but a loved one. It widened the divide, confirming I was walking an uncommon road with an uncommon child. But I never asked “why.” My heart stayed focused on “what.” What is this condition? What could we do? What help existed? What would life look like?
When the genetic counselor finally reached me one evening, I had paused my phone and was dancing with my boys to the Moana soundtrack. The lyrics hit me like waves. “When I cross that line, there’s no telling how far I’ll go.” In that moment, I knew — we would go far for this child. We would commit fully, even if it changed everything.
A prenatal hospice worker began visiting us, gently preparing us for loss. She showed burial gowns, memory boxes, hand molds, and quiet goodbyes. It felt compassionate — but it also nudged us constantly toward surrender. One afternoon, listening to her and my husband talk, I realized how much this path quietly assumed our daughter would not live. I placed research on the table showing children with Trisomy 18 do live — especially with proper interventions — and I said, “No more planning her death. She is alive.” That was the day I took charge.
Finding surgeons willing to help was another battle. Many said no — until one finally said, “I’ll take the kid.” He had operated on a child with T-18 years earlier and agreed to consider Rose. It was our first real “yes.” Still, I knew she needed a team — NICU doctors, specialists, people willing to stand beside her — not because she wasn’t fragile, but because she deserved the same chance as any baby.
Near delivery, I handed my new OB a detailed birth and after-care plan. Instead of rejecting it, she looked up and asked, “What’s our algorithm?” That word — our — changed everything. For the first time, I felt medicine turning toward partnership.
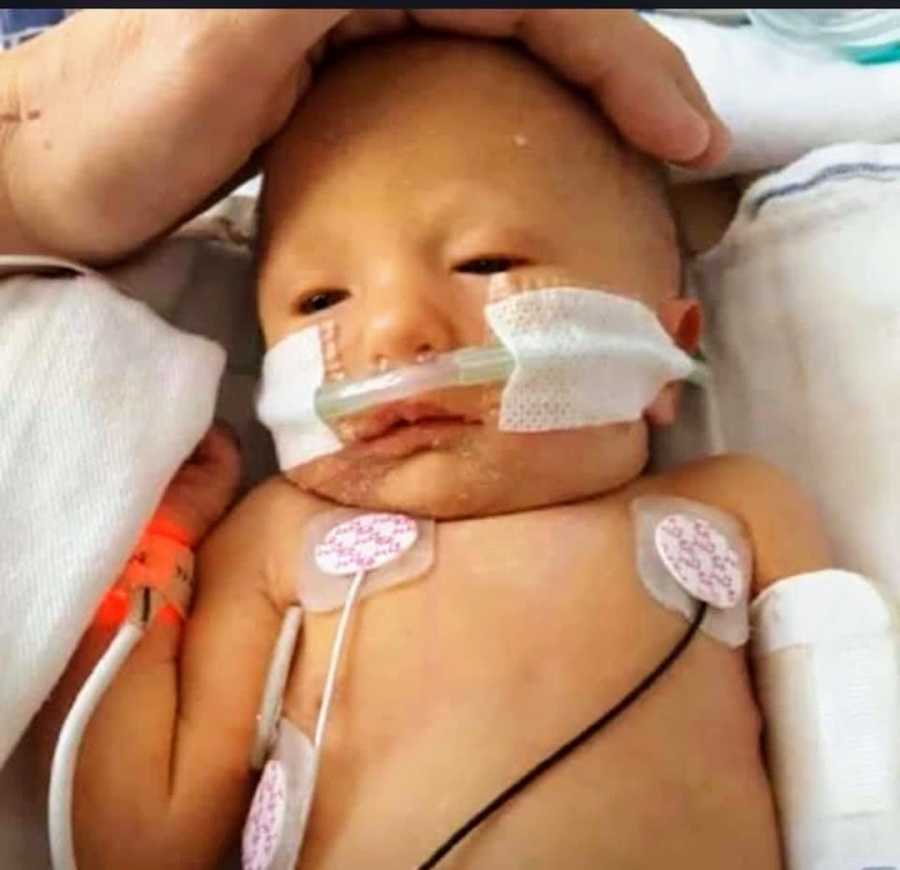
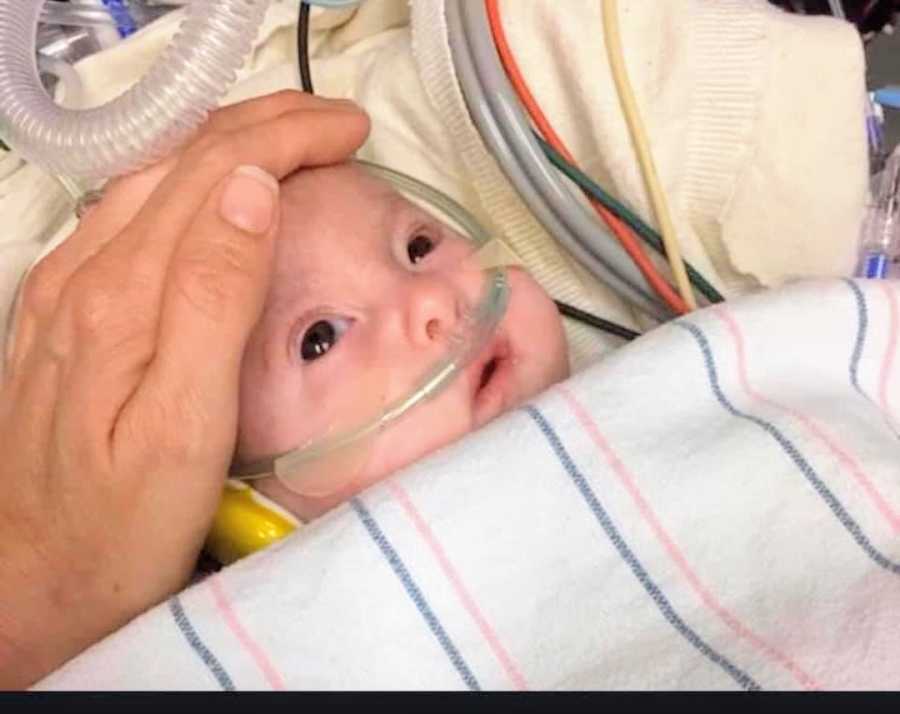
Rose’s first six weeks were intense. The system expected her to die. Instead, she responded to treatment — and lived. It scared and frustrated many staff members. I heard comments no mother should ever hear: refusals to re-intubate, dismissive remarks, judgments that we were being “cruel,” suggestions to “let her go.” We waited for heart repair, while they quietly waited for her to pass.
One night, I overheard a nurse joking about “how far” they should go for a T-18 baby. I confronted them — reminding them she was full code — then ran to the bathroom and vomited. I realized our supposed access to care was fragile — a house of cards.
Eventually, I learned they were considering “slow-code” measures — responding intentionally late in emergencies. That was the moment I knew we had to leave. I had gathered referrals months earlier, never imagining I’d use them — but suddenly, they were our lifeline.

Omaha Children’s Hospital accepted her. Insurance denied us twice; a judge overturned it after three exhausting days. Rose was medically transported alone — I wasn’t allowed to board. Our family packed, prayed, cried, and let her go into the sky. I promised I wouldn’t say goodbye — I would say hello when she landed.

She arrived in Omaha on March 22, 2018. Four days later, Dr. Hammel performed full heart repair. Today, Rose is a joyful toddler — loved, thriving, and proving every day that “incompatible with life” does not define her story.

We are endlessly grateful to those who believed she deserved fair care — and humbled that we get to help her live the beautiful life that once seemed impossible.








